IABP: Positioning with TEE
Goal is placement of IABP tip 1-2 cm distal to SCA takeoff
 The tip of the IABP catheter extends about 2 cm beyond the upper extent of the actual balloon, this placement allows for maximum augmentation of flow to the arch vessels (and coronaries) without compromising flow to the left subclavian artery (SCA).
The tip of the IABP catheter extends about 2 cm beyond the upper extent of the actual balloon, this placement allows for maximum augmentation of flow to the arch vessels (and coronaries) without compromising flow to the left subclavian artery (SCA).
High placement in the arch can decrease flow to the brain and upper extremities.
Low placement can interfere with flow to the renal and intra-abdominal arteries.
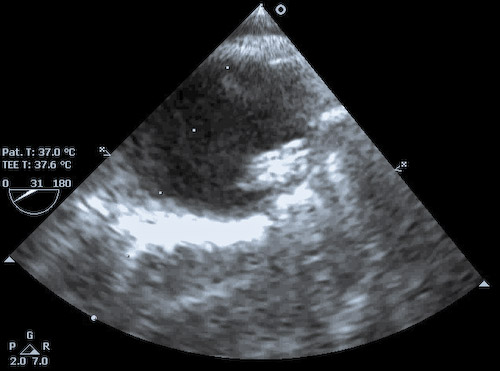
The figure to the left shows an IABP positioned slightly too high with the tip of the actual balloon just at the distal margin of the origin of the left SCA (visible from ~ 1-2 'o-clock). The IABP needs to be withdrawn in its femoral sheath by about 2-3 cm.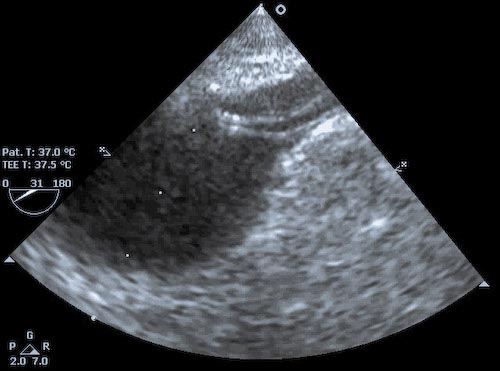
In the image to the right, the tip of the IABP actually lies within the SCA, thus must be withdrawn a significant distance.
Remember too that in the OR the patient may be positioned with legs flexed for vein harvest. Thus the IABP may well be pulled distally when the legs are returned to neutral. It is wise to recheck the position of the IABP with TEE prior to transport to the ICU.
Malpositioning of the IABP is NOT reliably detectable on the arterial waveform tracing - though low placement may show equalization of the IABP-assisted peak diastolic with the native-beat peak systolic pressure (which has other causes, eg: late inflation, balloon leaking, IABP too small for patient, or inflation volume set too low). Even when placed using echo guidance, it is imperative that IABP position be confirmed with CXR.
The still frame in the left upper corner of this page was taken in systole - with the balloon deflated - from the video to the left.
The IABP is positioned too high, as the SCA take-off is clearly visible, and partially occluded by the balloon.