IABP: Positioning with CXR
Goal is placement of IABP tip 1-2 cm distal to SCA takeoff
 As, unlike with echo, this position cannot be directly visualized, the radio-opaque marker on the tip of the IABP (which is beyond the balloon) is positioned using radiographic landmarks in a properly exposed chest film of a properly positioned patient.
As, unlike with echo, this position cannot be directly visualized, the radio-opaque marker on the tip of the IABP (which is beyond the balloon) is positioned using radiographic landmarks in a properly exposed chest film of a properly positioned patient.
The CXR on the left shows a common ICU x-ray: Poorly exposed, patient not properly positioned (though pretty good). With digital images, it is usually possible to adjust the contrast so that the essential landmarks can be seen. If you cannot see what you need, get the image re-shot. Here the IABP is too low, though you would be hard pressed to identify this.
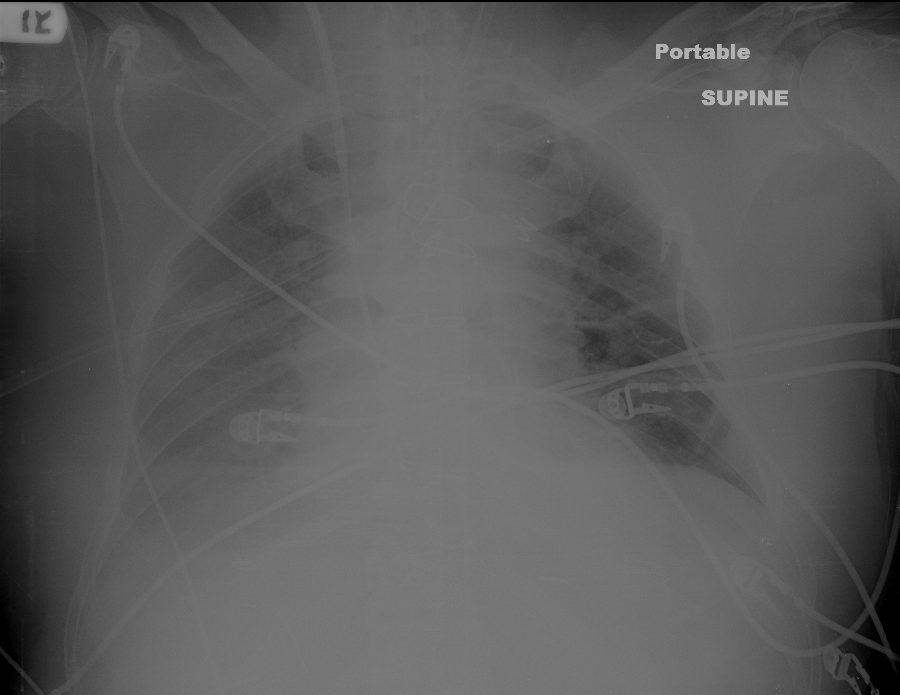
The image to the right is a better exposure for lines, but it is difficult to precisely identify the radiographic landmarks for IABP placement. Arrow points to IABP tip marker (vertical, white, ~2 cm long). Placement is still too low.
Radiographic landmarks for correct position vary somewhat by author. The most common is that the IABP tip marker should be 2cm below the top of the aortic knob; second most common is that the tip should be in the 2nd or 3rd intercostal space anteriorly. Either, or both, of these landmarks may be difficult to visualize in the typical ICU patient who needs a balloon.
Fortunately, most of these patients have a PAC in place. My suggestion is that if the other landmarks are difficult to see, simply place the tip of the IABP 1-2cm superior to the highest point on the PAC as it passes through the right (usually) or left PA. most of these patients have a PAC in place. My suggestion is that if the other landmarks are difficult to see, simply place the tip of the IABP 1-2cm superior to the highest point on the PAC as it passes through the right (usually) or left PA.
The anatomic drawing from Gray's Anatomy makes this relationship clear.
If seen, the aortic knob is likely the best. If knob not visualized well, the PAC method is probably the next best. The interspace method suffers from the width of the interspace's, and from the large geometric change with changing patient position.
Even if placed using fluoroscopic guidance, it is best that IABP position be documented with CXR.
IABP position should be confirmed by CXR at least once a day, whenever it is repositioned, and whenever it might have accidentally been moved, as malpositioning can kill the brain, bowel, kidneys, or patient. |